


Treatment Options
Choosing Surgery
Weight loss surgery is major surgery. Although most patients enjoy an improvement in obesity-related health conditions (such as mobility, self-image and self-esteem) after the successful results of weight loss surgery, these results should not be the overriding motivation for having the procedure. The goal is to live better, healthier and longer.
That is why you should make the decision to have weight loss surgery only after careful consideration and consultation with an experienced bariatric surgeon or a knowledgeable family physician. A qualified surgeon should answer your questions clearly and explain the exact details of the procedure, the extent of the recovery period and the reality of the follow-up care that will be required. They may, as part of routine evaluation for weight loss surgery, require that you consult with a dietician/nutritionist and a psychiatrist/therapist. This is to help establish a clear understanding of the post-operative changes in behavior that are essential for long-term success.
It is important to remember that there are no ironclad guarantees in any kind of medicine or surgery. There can be unexpected outcomes in even the simplest procedures. What can be said, however, is that weight loss surgery will only succeed when the patient makes a lifelong commitment. Some of the challenges facing a person after weight loss surgery can be unexpected. Lifestyle changes can strain relationships within families and between married couples. To help patients achieve their goals and deal with the changes surgery and weight loss can bring, most bariatric surgeons offer follow-up care that includes support groups, dieticians and other forms of continuing education.
Ultimately, the decision to have the procedure is entirely up to you. After having heard all the information, you must decide if the benefits outweigh the side effects and potential complications. This surgery is only a tool. Your ultimate success depends on strict adherence to the recommended dietary, exercise and lifestyle changes.
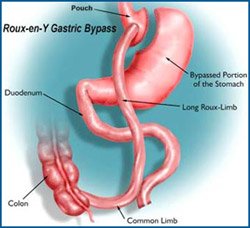
Roux-en-Y Gastric Bypass
 According to the American Society for Bariatric Surgery and the National Institutes of Health, Roux-en-Y gastric bypass is the current "gold standard" procedure for weight loss surgery. It is one of the most frequently performed weight loss procedures in the United States.
According to the American Society for Bariatric Surgery and the National Institutes of Health, Roux-en-Y gastric bypass is the current "gold standard" procedure for weight loss surgery. It is one of the most frequently performed weight loss procedures in the United States.
In this procedure, stapling creates a small (15 to 20cc) stomach pouch. The remainder of the stomach is not removed, but is completely stapled shut and divided from the stomach pouch. The outlet from this newly formed pouch empties directly into the lower portion of the jejunum, thus bypassing calorie absorption. This is done by dividing the small intestine just beyond the duodenum for the purpose of bringing it up and constructing a connection with the newly formed stomach pouch. The other end is connected into the side of the Roux limb of the intestine creating the "Y" shape that gives the technique its name. The length of either segment of the intestine can be increased to produce lower or higher levels of malabsorption.
Roux-en-Y Advantages
- The average excess weight loss after the Roux-en-Y procedure is generally higher in a compliant patient than with purely restrictive procedures.
- One year after surgery, weight loss can average 77% of excess body weight.
- Studies show that after 10 to 14 years, 50-60% of excess body weight loss has been maintained by some patients.
- A 2000 study of 500 patients showed that 96% of certain associated health conditions studied (back pain, sleep apnea, high blood pressure, diabetes and depression) were improved or resolved.
Roux-en-Y Risks
- Because the duodenum is bypassed, poor absorption of iron and calcium can result in the lowering of total body iron and a predisposition to iron deficiency anemia. This is a particular concern for patients who experience chronic blood loss during excessive menstrual flow or bleeding hemorrhoids. Women, already at risk for osteoporosis that can occur after menopause, should be aware of the potential for heightened bone calcium loss.
- Bypassing the duodenum has caused metabolic bone disease in some patients, resulting in bone pain, loss of height, humped back and fractures of the ribs and hip bones. All of the deficiencies mentioned above, however, can be managed through proper diet and vitamin supplements.
- A chronic anemia due to Vitamin B12 deficiency may occur. The problem can usually be managed with Vitamin B12 pills or injections.
- A condition known as "dumping syndrome" can occur as the result of rapid emptying of stomach contents into the small intestine. This is sometimes triggered when too much sugar or large amounts of food are consumed. While generally not considered to be a serious risk to your health, the results can be extremely unpleasant and can include nausea, weakness, sweating, faintness and, on occasion, diarrhea after eating. Some patients are unable to eat any form of sweets after surgery.
- In some cases, the effectiveness of the procedure may be reduced if the stomach pouch is stretched and/or if it is initially left larger than 15-30cc.
- The bypassed portion of the stomach, duodenum and segments of the small intestine cannot be easily visualized using X-ray or endoscopy if problems such as ulcers, bleeding or malignancy should occur.
- Additional risks include anastomotic leaks, deep vein thrombosis, pulmonary embolism, marginal ulceration, intestinal obstruction, and bleeding which may or may not require a transfusion.
Minimally Invasive Approach
During the procedure, surgeons usually use laparoscopic techniques (using small incisions and long-shafted instruments rather than a large incision), to implant an inflatable silicone band into the patient's abdomen. Like a wristwatch, the band is fastened around the upper stomach to create a new, tiny stomach pouch that limits and controls the amount of food you eat. It also creates a small outlet that slows the emptying process into the stomach and the intestines. As a result, patients experience an earlier sensation of fullness and are satisfied with smaller amounts of food. In turn, this results in weight loss.
Least Traumatic Procedure
Since there is no cutting, stapling or stomach rerouting involved in the Lap Adjustable gastric banding procedure, it is considered the least tramatic of all weight loss surgeries. The laparoscopic approach to the surgery also offers the advantages of reduced post-operative pain, shortened hospital stay and quicker recovery. If for any reason the gastric band needs to be removed, the stomach generally returns to its original form.
Adjustable Treatment
The diameter of the band is adjustable to meet your individual needs, which can change as you lose weight. For example, pregnant patients can expand their band to accommodate a growing fetus, while patients who aren't experiencing significant weight loss can have their bands tightened.
To modify the size of the band, its inner surface can be inflated or deflated with saline solution. The band is connected by tubing to a reservoir, which is placed well under the skin during surgery. After the operation, the surgeon can control the amount of saline in the band by entering the reservoir with a fine needle through the skin.
AGB Advantages
- Simple and relatively safe
- Short recovery period
- Major complication rate is low
- No opening or removal of any part of the stomach or intestines
- No altering of the natural anatomy
AGB Disadvantages/Complications
- Band erosion: The band can erode through the wall of the stomach. This results in loss of restriction to eating or infection caused by leakage of stomach juices onto the band. This erosion of the band almost always requires removal of the band, with plans for a later conversion to a different weight loss procedure.
- Band slippage or shifting: The band must remain in the correct position on the upper stomach in order to function properly. If it slips out of place or twists, it is likely to cause obstruction of the stomach, requiring fairly urgent re-operation to reposition the Band.
- Hardware breakage: The band, the port and the connection tubing are designed to last for life. In fact, the band itself is almost never reported to break or leak. However, the tubing and the port can become twisted, kinked or broken. Such events require re-operations (usually minor) for repair or repositioning of the problem spot.
- Weight loss: It should also be noted that weight loss with the lap band is generally lower than with the roux-en-y.
The LAP-BAND System is Patented and Copyrighted by Allergan. Realize® Band is protected by Ethicon. For more information, visit .
Sleeve Gastrectomy - Also known as Vertical Sleeve Gastrectomy (VSG), Vertical Gastrectomy
The newest of alternatives in weight loss surgery, the Sleeve Gastrectomy generates weight loss by restricting the amount of food (and therefore calories) that can be eaten by removing 85% or more of the stomach without bypassing the intestines or causing any gastrointestinal malabsorption. It is a purely restrictive operation. It is currently indicated as an alternative to the Lap-Band® procedure for low weight individuals and as a safe option for higher weight individuals.
Anatomy
 This procedure generates weight loss solely through gastric restriction (reduced stomach volume). The stomach is restricted by stapling and dividing it vertically and removing more than 85% of it. This part of the procedure is not reversible. The stomach that remains is shaped like a very slim banana and measures from 1-5 ounces (30-150cc), depending on the surgeon performing the procedure. The nerves to the stomach and the outlet valve (pylorus) remain intact with the idea of preserving the functions of the stomach while drastically reducing the volume. By comparison, in a Roux-en-Y gastric bypass, the stomach is divided, not removed, and the pylorus is excluded. The Roux-en-Y gastric bypass stomach can be reconnected (reversed) if necessary. Note that there is no intestinal bypass with this procedure, only stomach reduction. The lack of an intestinal bypass avoids potentially costly, long term complications such as marginal ulcers, vitamin deficiencies and intestinal obstructions.
This procedure generates weight loss solely through gastric restriction (reduced stomach volume). The stomach is restricted by stapling and dividing it vertically and removing more than 85% of it. This part of the procedure is not reversible. The stomach that remains is shaped like a very slim banana and measures from 1-5 ounces (30-150cc), depending on the surgeon performing the procedure. The nerves to the stomach and the outlet valve (pylorus) remain intact with the idea of preserving the functions of the stomach while drastically reducing the volume. By comparison, in a Roux-en-Y gastric bypass, the stomach is divided, not removed, and the pylorus is excluded. The Roux-en-Y gastric bypass stomach can be reconnected (reversed) if necessary. Note that there is no intestinal bypass with this procedure, only stomach reduction. The lack of an intestinal bypass avoids potentially costly, long term complications such as marginal ulcers, vitamin deficiencies and intestinal obstructions.
Comparison to prior Gastroplasties (stomach stapling of the 70-80s)
The Sleeve Gastrectomy is a significant improvement over prior gastroplasty procedures for a number of reasons:
- Rather than creating a pouch with silastic rings or polypropylene mesh, the Sleeve Gastrectomy actually resects or removes the majority of the stomach. The portion of the stomach which is removed is responsible for secreting Ghrelin, which is a hormone that is responsible for appetite and hunger. By removing this portion of the stomach rather than leaving it in-place, the level of Ghrelin is reduced to near zero, actually causing loss of or a reduction in appetite (Obesity Surgery, 15, 1024-1029, 2005). Currently, it is not known if Ghrelin levels increase again after one to two years. Patients do report that some hunger and cravings do slowly return. An excellent study by Dr. Himpens in Belgium(Obesity Surgery 2006) demonstrated that the cravings in a VSG patient 3 years after surgery are much less than in LapBand patients and this probably accounts for the superior weight loss.
- The removed section of the stomach is actually the portion that “stretches” the most. The long vertical tube shaped stomach that remains is the portion least likely to expand over time and it creates significant resistance to volumes of food. Remember, resistance is greatest the smaller the diameter and the longer the channel. Not only is appetite reduced, but very small amounts of food generate early and lasting satiety(fullness).
- Finally, by not having silastic rings or mesh wrapped around the stomach, the problems which are associated with these items are eliminated (infection, obstruction, erosion, and the need for synthetic materials). An additional discussion based on choice of procedures is below.
Alternative to a Roux-en-Y Gastric Bypass
The Vertical Gastrectomy is a reasonable alternative to a Roux en Y Gastric Bypass for a number of reasons:
- Because there is no intestinal bypass, the risk of malabsorptive complications such as vitamin deficiency and protein deficiency is minimal.
- There is no risk of marginal ulcer which occurs in over 2% of Roux en Y Gastric Bypass patients.
- The pylorus is preserved so dumping syndrome does not occur or is minimal.
- There is no intestinal obstruction since there is no intestinal bypass.
- It is relatively easy to modify to an alternative procedure should weight loss be inadequate or weight regain occur.
- The limited two year and 6 year weight loss data available to date is superior to current Banding and comparable to Gastric Bypass weight loss data(see Lee, Jossart, Cirangle Surgical Endoscopy 2007).
Low BMI individuals who should consider this procedure include:
- Those who are concerned about the potential long term side effects of an intestinal bypass such as intestinal obstruction, ulcers, anemia, osteoporosis, protein deficiency and vitamin deficiency.
- Those who are considering a Lap-Band® but are concerned about a foreign body or worried about frequent adjustments or finding a band adjustment physician.
- Those who have other medical problems that prevent them from having weight loss surgery such as anemia, Crohn’s disease, extensive prior surgery, severe asthma requiring frequent steroid use, and other complex medical conditions.
- People who need to take anti-inflammatory medications may also want to consider the Vertical Gastrectomy. Unlike the gastric bypass where these medications are associated with a very high incidence of ulcer, the VSG does not seem to have the same issues. Also, Lap-Band ® patients are at higher risks for complications from NSAID use.
All surgical weight loss procedures have certain risks, complications and benefits.
*Sleeve gastrectomy information from www.obesityhelp.com
* Image © Laparoscopic Associates of San Francisco
Risks of Surgery
Indications
Bariatric surgery is intended for people who are 100 pounds or more overweight (with a Body Mass Index of 40 or greater) and who have not had success with other, less risky weight loss therapies such as diet, exercise, medications, etc. In some cases, a person with a Body Mass Index (BMI) of 35 or greater and one or more co-morbid condition may be considered for bariatric surgery.
Important Considerations
Bariatric surgery should not be considered until you and a doctor have looked at all other options. The best approach to bariatric surgery calls for discussion of the following with your doctor:
- Bariatric surgery is not cosmetic surgery and should not be thought of in any way as cosmetic surgery.
- Bariatric surgery does not involve the removal of tissue (fat) by suction or surgical removal.
- The patient and doctor should discuss the benefits and risks together.
- The patient must commit to long-term lifestyle changes, including diet and exercise, which are key to the success of bariatric surgery.
- Problems after surgery may require more operations to correct them.
Complications of Bariatric Surgery
As with any surgery, there are immediate and long-term complications and risks. Your healthcare team can speak with you further about the benefits and risks. Possible risks can include, but are not limited to:
- Bleeding*
- Complications due to anesthesia and medications
- Deep vein thrombosis - Blood clots in the large leg veins. They become serious when they float up into the blood vessels of the lungs. Prevention methods include wearing compression stockings, taking blood thinners and walking as soon as possible after surgery.
- Hernia. One of the more common complications requiring another operation to fix
- Dehiscence (separation of areas that are stitched or stapled together)
- Infections
- Leaks from staple lines
- Marginal ulcers
- Pulmonary problems
- Spleen injury*
- Stenosis (narrowing of a passage, such as a valve)
- Death
* To control operative bleeding, removal of the spleen may be necessary.
We strongly advise you to involve your loved ones in the decision and education process about Weight Loss Surgery. In the end, the decision for surgery falls to the patient alone, but the entire process is definitely better for everyone if family support is strong.
Portions of the above content were taken from Ethicon Endo-Surgery, Inc.’s web site
Patient Forms
Bariatrics Patient Survey—Weight-loss surgery can change your health, and your life. If you are interested in more information about surgery and learning if you qualify for the procedure, please fill out the questionnaire attached and submit it based on the instructions.
Bariatrics Patient Packet—Once you are considered a potential candidate for surgery, you will be asked to fill out this Bariatrics Patient Packet. Please download the form and complete the form prior to your first visit with West Florida Weight Loss.
Bariatrics Fee—Information and form regarding the bariatric program fee for insurance patients.
Gastric Bypass Instructions / Consent Form—Prior to having Gastric Bypass Surgery you will asked to read the attached consent form and sign the document as to your understanding of the procedure that is being performed. This form may be download here. This form includes information about the operation, Expected Outcomes & Patient Commitments, Diet, Risk of Operation, Other Undesirable Outcomes, Fees, and a Summary.
Communication Release Form—A form authorizing Surgical Associates of West Florida to contact you. Form allows you to specify preferred method of communication, and other parties to whom your health information may be released.